

“CODE BLUE, 7 SOUTH. CODE BLUE, 7 SOUTH.” I’m up and out of my call room bed before fully regaining consciousness from my light sleep. It’s 4 AM. I should feel ready: I’ve trained with simulations labs, mock codes, and test questions. I passed my CPR and ACLS courses. I’ve done chest compressions as an intern. But this is different. I’m the resident on call, and if I get there first, I’ll be running the Code. I’ve never run one before. I’m terrified. I’m not ready.
Code Blue is essentially a euphemism for being dead. While it technically means “medical emergency,” it has come to mean that someone in the hospital has a heart that has stopped beating. The outcome statistics are grim. Even with perfect CPR, in hospital cardiac arrests have a roughly 85% mortality. Those that somehow survive are often left with irreversible brain damage and lie in comas. Few ever leave the hospital. Death is greedy.
Still, we have to try. I run down the corridor towards the patient’s bed. My sneakers make little squeaks against the linoleum floor, echoing off the walls of the mostly quiet hospital. My mind is a zoo. The flooring makes this place sound like a gymnasium. How many minutes in between epinephrine injections again? I should run more, I’m already out of breath. Think of causes, causes. The 5 H’s, the 4 T’s. What was the room number?
I burst into the room, out of breath. It is pure, primordial chaos. I’m hit with the sound first. Bed alarms, blood pressure alarms, and heart rate alarms blare insistently, a Greek Chorus to the unfolding drama. An unanswered, continuous string of questions hangs in the air like a heavy fog. “Can someone page anesthesia?” “Where’s the cards fellow?” “Do we need femoral access?” “Where’s the EKG?” “Chest X ray stat!” “Who spoke to the family?” “Is this guy DNR?” “Who has a hemoglobin?” “Is he on blood thinners?” “What’s his history?” I can hardly hear myself think. This must be what being in the cockpit of a nosediving plane is like.
I take stock of the room. One nurse is on the bed, performing chest compressions. A second is trying to steady the man’s arm to place an IV, but is having a hard time. A third is struggling to hold an oxygen mask to the man’s face while squeezing an amboo bag. Pharmacists are rifling through a large red chest of medications. Someone is desperately clicking at a frozen computer in the corner of the room. A gaggle of nurses, aids, and respiratory therapists stand at the door.
The patient is staring straight at me. His eyes are glazed and unfocused. He’s an older white man with a shaggy beard and sunken temples. His skin is a uniform, mottled blue-grey. His head flops every second or so from the force of the compressions, and currently he’s turned to face the door, looking at whoever crosses the threshold.
I take a deep breath. “Is anyone running this code?”
There is only silence. Beautiful, terrifying silence. No one is standing at the foot of the bed, which is where the code leader would normally stand. I’m going to have to run it. It’s only a second or two, but the moment stretches and stretches. And seconds matter.
The brain is the most adaptable and responsive piece of biological engineering we know of. It responds in real time to the binary input of billions of neurons to create sight, sound, and sensation. It can accommodate elevation changes, pH changes, temperature changes, volume changes, infectious states, starvation, and fight-or-flight responses. But it has an insatiable demand for oxygen. There is no safe-mode, no low power state. Four minutes without oxygen destroys seventy-six years of life. Here we go.
“I’m Dr. Gold, I’m leading this code. You, keep time. You, continue compressions. Let’s hook up the pads. Draw up one milligram of epinephrine…”
The training kicks in hard. Good hard chest compressions, with epinephrine every 2-5 minutes. Pulse checks every 2 minutes. Shock the heart if it’s ventricular tachycardia or ventricular fibrillation – a call that will be made by me. I hear a faint crinkling sound with every compression. Ribs breaking. Then a voice: “2 minutes, doctor.”
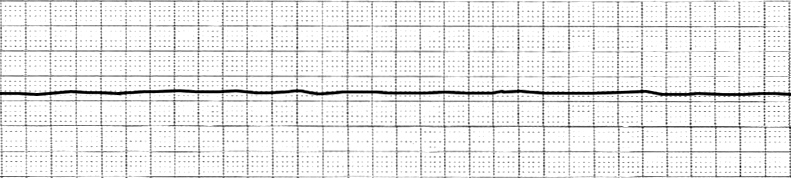
“Pulse check!” The compression stop. Hands immediately reach for the femoral and carotid arteries, straining to feel the reassuring rhythmic pulse of life. All eyes turn to the cardiac monitor. It’s hard to interpret while compressions are going, but now it’s clear. The heart’s electrical system normally conducts each beat with fanatical precision:

Now it is in disarray, starved from a lack of oxygen:

It’s V-Fib. Disorganized, random electrical discharge that is unable to produce heartbeats. “It’s V-fib.” I say it quietly, almost to myself. No one moves. “V-fib,” I say again louder. Still nothing. Why aren’t they moving? Oh, right. They’re waiting for me to say something. “Continue compressions. Charge the defibrillator. We’re going to shock.”
We shock. The patient’s body tenses suddenly and violently. It’s strange to see him move so much. Strange that our muscles run on electricity. Strange that to save someone you hook them up to an outlet. We’re more machine than we realize. To reset pacemaker: turn it off, turn it on, see if that helps.
We continue CPR. Anesthesiology comes and inserts a tube into his throat so we can breath for him. But it doesn’t matter. We never get another shockable rhythm after the first shock, just a flat line. Asystole.
More compressions. More epinephrine. Other meds, too: amiodarone, calcium, magnesium, bicarbonate. We draw quick-resulting labs. We call cardiology for a bedside echocardiogram to look at the heart. It’s not moving at all. After 30 minutes, I ask if anyone has any objections to stopping the code. No one does.
We pronounce him dead.
And just like that, the mayhem ends. The compressions stop. The plastic IV tubes are disconnected and thrown out. The hastily placed endotracheal tube is removed. The alarms are silenced. The defibrillator pads are removed. Pharmacy takes their cart of medications and leaves. The crowd begins to thin.
The patient’s nurse begins making the final arrangements before the family arrives. His jaw, which was slightly gaping, is gently closed. His head is laid straight back, eyes looking up. Bloody linens are replaced with fresh ones. The patient is draped in a new gown.
Despite his recent ordeal, the patient now radiates a sense of calm. The man’s stillness is serene, otherworldly. Impossible for a living being to achieve. The few remaining people in the room use hushed voices. The room feels sacred, somehow. I look at the man again. I think of Homer’s line from the Odyssey: “Upon his eyes gathered the mist of death.”
I perform the death exam. I check his eyelids and see no corneal reflex. Feel no pulse. Hear no breath sounds. It’s done. I exit the room.
A few feet from the door, a young black woman in cheery pink scrubs is curled up in a ball on a rolling chair near a desk. Her head is in her hands. Her shoulders jerk intermittently. In printed block letters, her ID badge reads MEDICAL VOLUNTEER.
I ask if she’s OK, and she looks up at me. Her eye shadow is starting to streak down around the corners of her eyes.”I was watching him. I – I called for help. He wasn’t breathing. I’ve never seen… that… before.”
I nod. Words don’t come. I stand beside her for a while. After a few minutes, I turn and head back to my call room. Somehow, I feel comforted by her crying. This seems the most appropriate reaction to the last thirty minutes of anyone.
I’ve run a few more codes since this one. It feels, if not routine, certainly easier than the first one. More algorithmic. But I can’t shake the feeling that I shouldn’t become too comfortable doing this. I want to always remember that volunteer. She didn’t know this patient personally, it wasn’t family. But she wept all the same. To me, her tears acknowledged the frailty of it all, the randomness. The callousness of death, the gift that is life. It was inspiring. The day I can’t feel the way she does about my patients is the day I need to find a new profession.
I always knew you would be a great Dr. You have compassion, don’t ever lose it, no matter how hard it gets.
I appreciate the humanity in your post. As a medical student, I want to hold onto my compassion for patients and their families, especially after tragedy. Thank you for acknowledging her feelings and taking a moment to stand with her. I’m sure that affected her for the better.
Absolutely fantastic. Such a surreal and real depiction of a code and of watching death. It is a reminder to us all of the need for humanity in the medical field. I feel sure that you are wonderful doctor and teacher. Thank you and good luck.
This is absolutely beautiful Ben and brought tears to my eyes. We are so proud of the caring, compassionate, honest Renaissance man that you are. Love you honey- mom
Love this message from Mom
Good writing ! I appreciate all the little details
Great post. I can feel the emotion in this.
You’re young and you don’t know everything and you are especially wrong about opiates and it is sad you won’t prescribe them to patients in horrible pain and who need their jobs.
I feel their pain as a long time, long term pain sufferer who has had opiates off and on and am extremely grateful doctors did not treat me as an addict and I have never been addicted.
I have a husband who is an ER physician (MIT, UMich graduate) and I graduated (Amherst ’98 and Howard Law 02 all while having SLE -1988 and chronic daily migraines -1993)… there was no topamax in 1993.
I have two happy, smart kids ages 8 and 12…a good home and life… but the moral of this tale is to say it’s sad the new breed of physicians are taking the tales of all who have become addicts and letting those in pain who need treatment suffer.
Should we conflagrate and inflate every instance a medical professional has become addicted and thus highly monitor him/her…(If you lived in Houston long enough you would know about Dr. Brown the famous hand dr who became addicted to all types of drugs)…
It could be said that you and other physicians by withholding necessary treatment are violating the Hippocratic oath by refusing to relieve the real and enduring, awful pain of patients. That harms the patient. I will seek to do what I can to remedy and keep this from happening to future patients across this nation.
Tracey Valencia
You should watch Learning to code – Medicine the Musical
I’m a medical student in the finale year. I’ve meet a resident once, and asked her about (who should run the code?), she answered the first available person, even if that is a resident year 1. which is me one year and a half from now. all the things I found to learn about code blue were algorithms and step by step teaching of running it, there was nothing about what would you feel! if the end was not the desired end, “until your story mentioned in here”.
as students we hope for the better endings for the patient and study purely about he conditions and their diagnosis, but the devastating events are not mentioned, until we are going to be the first to deal with them during residency.
Thank you for sharing your story and best of luck.